Critères diagnostiques de recherche (RDC)
Critères diagnostiques de recherche (RDC)
A frequent feature of orofacial pain is the multifactorial nature of the pathology which makes the diagnosis even more complex. The Temporo Mandibular Disorders (TMD), for example, which the Anglo-Saxon countries call with various terminologies such as Temporo-Mandibular Disorders (TMDs), Cranio Facial Pain (CFP) and Temporo-Mandibular Joint Dysfunction (TMJ dysfunction), sometimes present diagnostic difficulties. The orofacial pain caused by DTM is often superimposed, as symptoms and clinical signs, on pain disorders that can be a manifestation of other forms of headache in which organic neurological-systemic pathologies can coexist. This clinical picture can make differential diagnosis difficult at least in the early stages of the disease.[1][2][3][4]
For this reason, numerous studies have followed to determine a standardized diagnostic evaluation method called Research Diagnostic Criteria (RDC). Atypical Orofacial Pain (ADO), is considered a broad group of facial pain disorders and is described as burning mouth, muscle cramps that occur on one side of the face and often in the trigeminal nerve territory. This symptomatology can extend to the cervical region and back of the head. The causes of the disease can be many and it has also been considered a "pathology of psychiatric competence".
A critical obstacle in understanding TMDs has been the loss of standardized diagnostic criteria for defining subtypes of TMDs. Therefore, it was decided to give life to a project to eliminate the lack of diagnostic and therapeutic standardization called Research Diagnostic Criteria and signed in the RDC.
Research Diagnostic Criteria
This called project requires that the repeatability and validity of the diagnostic criteria allow:
- The generation of clinical case definitions with reproducibility between clinicians and researchers
- Identification and assessment of etiologic, preventive, and risk factors as well as assessment of associated characteristics that initiate, prevent, maintain, or exacerbate the disorders
- Allow prognostic studies
- Establish effective treatment
The empirical data used to develop 'RDC' came from longitudinal epidemiological research supported by the National Institute for Dental Research (NIDR) and conducted at the University of Washington and the Group Health Corporation of Puget Sound, Seattle, Washington.
Samuel F. Dworkin, M. Von Korff and L. LeResche were the principal investigators.
In order to arrive at the formulation of the 'RDC' protocol, a literature review of the diagnostic methods in the DTMs was carried out and subjected to validation and reproducibility. Taxonomic factors were also considered but not uncritically.
The taxonomy of diseases, in fact, has developed because the classification of diseases is considered a useful way to improve knowledge of what would otherwise have been a confusing set of information. The taxonomy, however, is in itself a constructor or a set of constructors, and for this they need an evaluation referable to critical factors such as reliability and validation. For a diagnostic manufacturer to be considered valid, it must contain a series of valid disease descriptors. The disease descriptor is considered valid if and only if it is frequently found in patients with the disease and rarely observed in individuals without the disease.
Nine taxonomic systems were taken into consideration, that of Farrar (1972)[5]Block (1980)[6], Eversole e Machado (1985)[7], Bell (1986)[8], Fricton (1988)[9],American Academy of Craniomandibular Disorders (AACD) (1990)[10], Talley (1990)[11], Bergamini e Prayer-Galletti (1990)[12],Truelove (1992)[13], and compared, according them to a series of evaluation criteria. Some of these criteria can be applied in evaluating that builder or taxonomic system while others were developed by the authors themselves. The evaluation criteria have been divided into two categories that involve
- Methodological considerations
- Clinical considerations.
At the end of the research there was a drastic elimination of a series of instrumental diagnostic methodologies, due to lack of scientific and clinical validation (table 1)
| Table 1: DTM diagnostic methodologies analyzed and eliminated from the DRC because they are not scientifically validated | ||||
| Diagnostic Tests | Cutoff | Sensitivity | Specificity | VPP |
| Movimenti mandibolari e cicli masticatori | ||||
| Mandibular opening width (Dworkin et el.,1990)[14] | Males:35 mm
Females::30mm |
0.21
0.21 |
0.97
0.97 |
0.58
0.55 |
| Mandibular movement speed (Cooper e Rabuzzi, 1984)[15] | 300 mm/sec | - | 0.24 | - |
| Mandibular movement speed (Feine et al., 1988 )[16] | 250 mm/sec | 1.0 | 0.20 | 0.15 |
| Anterior/Posterior relationship (Feine et al., 1988)[16] | 1/2 | 0.86 | 0.30 | 0.14 |
| Masticatory cycles(Feine et al., 1988)[16] | descrittivi | 0.26 | 0.70 | 0.11 |
| Pantographic Reproducibility Index | ||||
| IRP (Shields et al.1978)[17] | 10 unità | 0.89 | 0.30 | 0.15 |
| Temporomandibular joint | ||||
| Digital palpation (Dworkin et al.,1990 )[14] | Presenza di click | 0.43 | 0.75 | 0.19 |
| Electrical stimulation methods | ||||
| Free rest space before stimulation( Cooper e Rabuzzi 1984)[15] | 0.75-2.0 mm | 0.42 | 0.62 | 0.17 |
| Free space to rest after electric-stimulation ( Cooper e Rabuzzi 1984;[15]) | 0.75-2.0 mm | 0.76 | 0.19 | 0.11 |
| Closure trajectory before after electrical stimulation( Cooper e Rabuzzi 1984)[15] | Non definita | 0.75 | 0.27 | 0.12 |
| Electromyography | ||||
| EMG at rest ( Cooper e Rabuzzi 1984)[18] | EM1=10μ V
EM2= 2.5μ V |
0.89 | 0.19 | 0.13 |
| Level of maximum masticatory closure | 160μ V | - | - | - |
| Cutoff: Parameters and limits of significance that should divide sick from healthy, for each test reportedSensitivity: Ability of the specified test to identify the truly sick in a sample of healthy and sick subjects
Specificity: Ability of the specified test to identify the healthy in a sample of healthy and sick subjects Positive Predictive Value (PPV): Ratio of the ability of the specified test to identify truly sick (positive) patients on the total sick population in a sample of healthy and sick subjects. | ||||
Without going into statistical topics, which we will deal with in specific chapters in the 'Extraordinary Science' section, we can observe, from the table, that the PPV, one of the essential components for scientific-clinical validation, is low for all diagnostic systems except for the method of measuring the jaw opening. The purpose of the RDC was precisely to provide a standardized criterion for research proposals based on the current state of knowledge regarding DTMs. For example, words such as 'often' or 'rarely' or 'limited jaw opening' have been eliminated and replaced with precise measurements such as '35mm opening'. The RDC was built on two axes:
Axis I corresponding to the clinical diagnosis Axis II corresponding to the psychophysical conditions in the patient with chronic pain.
The Axis I diagnostic scale is divided into 3 groups:
- Group I: Muscle diagnosis
- Myofascial pain
- Myofascial pain with limitation of jaw opening
- Group II: Meniscal dislocation
- Meniscal dislocation with reduction
- Meniscal dislocation without reduction with limited mandibular opening
- Meniscal dislocation without reduction and without limitation of mandibular opening
- Group III: Arthralgias, arthritis and osteoarthritis
- Arthralgia
- Osteoarthritis of the temporomandibular joint (TMJ)
- TMJ osteoarthritis
Quantification and classification of global severity of pain conditions were reported in Axis II. These conditions match:
- pain intensity.
- disability of the subject according to the pain pathology
- depression
- nonspecific physical symptoms.
Sparing the reader the RDC questionnaire consisting of 31 questions plus group and subgroups of questions, and the anamnestic file which considers functional aspects of the masticatory system such as the degree of jaw opening, deviation, ATM noises and symptomatic aspects, such as the localization of painful muscles on palpation, etc., to limit ourselves to describing and drawing conclusions on the fundamental principles on which the RDC is based.
Axis I: Clinical conditions of the DTM.
The first argument was that ambiguous terms should be avoided in the 'RDC'. In fact, many terms used to describe clinical conditions are used loosely. Spasm, according to Lund[19] contracture, contraction, hyperactivity, tension are some ambiguous terms. Diagnostic criteria for muscle spasm, myositis and contractures can be found in the medical literature. For example, myositis is characterized by weakness, EMG abnormalities recorded with needle electrodes, an elevated erythrocyte sedimentation level, an elevated serum creatine phosphokinase (CPK) level, and obvious inflammation on biopsy. In the proposed classification system, patients are assigned to three distinct groups: group I muscle conditions; group II meniscal dislocation; Group III arthralgias, attritis and osteoarthritis, on the basis of simple anamnestic examinations. Some believe, according to Lund, that myofascial pain and fibromyalgia can be distinguished by the presence of trigger points in the latter condition; others suggest that trigger points may be indistinguishable. One person's trigger point may, however, be another's tender point.
Subgroups I and II are defined on the basis of mouth opening. This clinical sign is under continuous discussion and should be related to gender and age. This can help improve the low predictive value associated with the 35mm cutoff. Widmer cites two studies reporting differences of 2.5 and 3.5 mm between sexes. The cutoff for maximum unassisted opening is different between groups I and II (40mm vs 35mm) as are the limits of painless passive stretching (>5mm vs 4mm). The reason for choosing different limits is not explained and the decision is not surprising. Mechanical factors, in fact, limit movement in Group II, while pain is the primary cause in Group I, but it would not be equally surprising if the subject could be classified in Group I one day and in Group II thereafter.
Pain measurement is part of the Axis II and being an important variable it should be considered using a continuous scale such as the visual analogue scale (VAS) or a verbal descriptive checklist (VDCL) topics that we have already discussed in the chapters on medical language logic.
The DTM questionnaire includes three questions related to the degree of pain; one for recent pain (n°7); one, for maximum pain in the last 6 months (n°9); one, for the average pain in the last 6 months (n°10). Interpretation, as can be guessed, remains very difficult as the patient's memory of pain is very low in the headache periods. The four questions on disability (n°11 to n°14) referring to the patient's memory could be more effective than the pain symptom, as it is easier to control the absence from work caused by the pain than the intensity of the pain itself. The authors recommend that depression, vegetative and physical phenomena be quantified using the SCL-90-R scale (a psychometric assessment tool by Leonard R. Derogatis).
Conclusions
The DRC was an obligatory step in defining guidelines capable of stemming the chaotic phenomenon of individual interpretation of the DTMs. In USA. in fact, the insurance system found itself displaced by the enormous health expenditure due to the improper interpretation of the data resulting from instrumental tests and clinical diagnostic methods that were not validated in the field of DTM. In fact, prosthetic, orthodontic, orthodontic-postural rehabilitation and, in any case, very expensive therapies were often indicated to these patients as therapy.
Unfortunately, the rigorous RDC system can only direct the diagnosis towards a more appropriate category but not define it with the same rigor and certainty, especially when it comes to defining a differential diagnosis between DTM and DOF caused by organic neurological or systemic pathologies which in the first phase of disease can manifest with widespread pain symptoms and/or comparable to a clinical manifestation such as TMD.
Another criticism that can be leveled at the 'RDC' is to consider the patient with TMD as a separate category almost exclusively dental and not as a pain subject at risk. This criterion focuses the diagnostic models on specifically dental requirements and excludes a series of clinical-instrumental diagnostic models which have a wider range of action.
The DRC's decision to completely eliminate instrumental scientific support in medical diagnostics has led to a clinical knowledge restriction on the part of doctors and dentists such that it is no longer possible to formulate an early differential diagnosis in headaches in which the damage is organic.
It can therefore be affirmed and confirmed that the CDR is not only restrictive but can sometimes be dangerous for the dentist because he can make himself responsible for inexperience. With this statement we do not want to cancel all the efforts made by the 'RDC' in order to give diagnostic and therapeutic limits and consequently considerably reduce speculation on the disease, but it is necessary to match this diagnostic model, mainly dental, with a vision more global medical semeiotics including the use of instrumental investigations.
In the next chapters, therefore, the basic elements of the 'RDC' will be discussed individually in order to be able to better evaluate the limits and advantages of this diagnostic model but before starting we present two emblematic clinical cases for the continuation of the chapters on the 'RDC' which induce a deep reflection on the subject.

Figure 1: Myasthenic case report considered TMD despite the mouth opening being greater than 40mm but presenting difficulty in chewing such as to lead the dental colleagues to makeover more mobile prostheses with increased vertical dimensions. After 2 months from the initial symptoms, the situation worsened with the appearance of a difficulty in swallowing. Some neurological clinical tests resulted positive: Mingazzini, index-nose, nystagmus, alteration of the swallowing reflex. These anamnestic data directed the diagnosis towards an organic neurological pathology. Subsequent laboratory tests (blood chemistry, Rx, trigeminal electrophysiological and repetitive stimulation) made it possible to formulate the diagnosis ofSindrome Miastenica di Eaton-Lambert (SMEL).

Figure 2: Post-polio syndrome was previously diagnosed with TMD and Occlusal-Postural disorder in reference to orofacial pain and vertigo phenomena despite the mandibular opening being greater than 40 mm. The anamnesis reported only an interesting correlation between the pain side and poliomyelitis contracted in childhood. On needle electromyographic examination of the temporal muscle, the recorded potentials showed a neuropathic picture with spontaneous activity, motor units of abnormal amplitude (> 2 mV) attributable to neuropathic suffering and reinnervation phenomena. The previous illness and the EMG examination led to a diagnosis of 'Post-polio syndrome'.
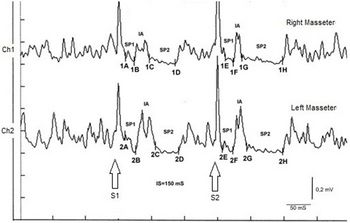
Figure 3: Bruxist patient classified in the RDC protocol in group I,2 Rifascial pain with limitation of mouth opening. Definitive diagnosis 'Cavernosa Pineal'



The images shown are only a part of the clinical cases that will be presented during the drafting of masticationpedia so the reader should know that Masticationpadia is a dynamic encyclopaedia and, therefore, over time the chapters of other information useful for understanding the rationale of the project which is first of all to observe the epochal clinical reality in masticatory rehabilitation, to observe the anomalies and possibly the crisis of the paradigm to then propose a new paradigm denominated following the Khunian settings 'Extraordinary Science' in which the International Scientific Community can focus its attention and constructive criticism.

- ↑ Sollecito T.P., Richardson R.M., Quinn P.D., Cohen G.S.:. Intracranial schwannoma as atypical facial pain. Case report. Oral Surg Oral Med Oral Pathol. 1993;76:153-6
- ↑ Shankland W.E.: Trigeminal neuralgia: typical or atypical? Cranio. 1993;11:108-12.
- ↑ Graff-Radford S.B., Solberg W.K.: Is atypical odontalgia a psychological problem? Oral Surg Oral Med Oral Pathol. 1993;75:579-82.
- ↑ Ruelle A., Datti R., Andrioli G.: Cerebellopontine angle osteoma causing trigeminal neuralgia: case report.Neurosurgery. 1994;35:1135-7.
- ↑ Farrar WB.: Differentiation of temporomandibular joint dysfunction to simplify treatment (other articles included) J.Prosthetic Dent. 1972; 28: 555-629
- ↑ Block SL.: Differential diagnosis of cranial facial cervical pain. In Sarnat BG:, Laskin DM (eds): The temporomandbular joint, ed 3. Springfield.III Charles C.Thomas .1980 pp. 348-421
- ↑ Eversole LR., Machado L.: Temporomandibular joint internal derangements and associated neuromuscular disorders. J. Am.Dent Assoc 1985; 110: 69-79
- ↑ Bell WE.: Temporomandibular disorders:Classification, Diagnosis, Management.(2 ed).Chicago Year Book Medical Publishers, 1986
- ↑ Fricton Jr., Kroening RJ., Hathaway KM.:TMJ and Craniofacial pain: Diagnosis and Management. St Louis, Ishiyaku EuroAmerica. 1988
- ↑ American Academy of Craniomandibular Disorders: Craniomandibular Disorders: Guidilines for evaluation, Diagnosi, and Management. Chicago, Quintessence Publ.Co 1990
- ↑ Talley Rl., Murphy GJ., Smith Sd., Baylin MA., Haden JL.: Standards for the history, examination, diagnosis, and treatment of temporomandibular disorders (DTM): A position paper. J Craniomand. Prat. 1990; 8: 60-77
- ↑ Bergamini M., Prayer-Galetti S.: A classification of musculoskeletal disorders of the stomatognatic apparatus. Front Oral Physiol. 1990; 7: 185-190
- ↑ Truelove EL., Sommers EE., LeResche L., Dworkin SF., Von Korff M.: Clinical diagnostic criteria for RMD: New classification permits multiple diagnosis. J. Am. Dent. Assoc. 1992; 123: 47-54
- ↑ 14.0 14.1 S F Dworkin, L LeResche, M R Von KorffDiagnostic studies of temporomandibular disorders: challenges from an epidemiologic perspective.Anesth Prog. 1990 Mar-Jun;37(2-3):147-54.
- ↑ 15.0 15.1 15.2 15.3 BC Cooper, D D Rabuzzi. Myofacial pain dysfunction syndrome: a clinical study of asymptomatic subjects. Laryngoscope. 1984 Jan;94(1):68-75. doi: 10.1002/lary.5540940116.
- ↑ 16.0 16.1 16.2 TT Dao, J S Feine, J P Lund. Can electrical stimulation be used to establish a physiologic occlusal position? J Prosthet Dent. 1988 Oct;60(4):509-14.doi: 10.1016/0022-3913(88)90259-4.
- ↑ James M. Shields, Joseph A. Clayton, Larry D. Sindledecker. Using pantographic tracings to detect TMJ and muscle dysfunctions. J Prosthet Dent.Volume 39, Issue 1, P80-87, January 19788
- ↑ Barry C. Cooper D.D.S., Daniel D. Rabuzzi M.D.Myofacial pain dysfunction syndrome: A clinical study of asymptomatic subjects. Laryngoscope. January 1984 https://doi.org/10.1002/lary.5540940116
- ↑ Lund JP., Widmer CG., Donga R., Stohler CS.: The pain adaptation model: An explanation of the relationship between chronic pain and musculuar activity. Can J Physiol Pharmacol 1991; 69: 683-694